 After a recent reminder from the U.S. Patent and Trademark Office (USPTO) regarding the duties of disclosure and reasonable inquiry during examination of a patent application and a Request for Comments (RFC) on the USPTO initiatives to ensure “robustness and reliability” of patent rights,[1] the Director of the U.S. Patent and Trademark Office published a third notice in less than four months. The latest notice is in conjunction with the Food and Drug Administration (FDA) to further the discussion surrounding the patent practices of the pharmaceutical industry (87 Fed. Reg. 67019 (November 7, 2022)). Specifically, the notice is of a public listening session and request for comments (PLS/RFC).
After a recent reminder from the U.S. Patent and Trademark Office (USPTO) regarding the duties of disclosure and reasonable inquiry during examination of a patent application and a Request for Comments (RFC) on the USPTO initiatives to ensure “robustness and reliability” of patent rights,[1] the Director of the U.S. Patent and Trademark Office published a third notice in less than four months. The latest notice is in conjunction with the Food and Drug Administration (FDA) to further the discussion surrounding the patent practices of the pharmaceutical industry (87 Fed. Reg. 67019 (November 7, 2022)). Specifically, the notice is of a public listening session and request for comments (PLS/RFC).
Against the backdrop of President Biden’s Competition Executive Order (EO) that calls for action “to help ensure that the patent system, while incentivizing innovation, does not unjustifiably delay generic drug or biosimilar competition beyond that reasonably contemplated by applicable law,” as well as Congressional and public interest in this goal, the stated purpose of the present notice of the PLS/RFC is to obtain public input for areas of joint USPTO-FDA collaboration and engagement with respect to the pharmaceutical industry to promote greater access to medicines for American families.
In particular, the USPTO and FDA are seeking feedback from a broad group of stakeholders, most notably, patients and their caregivers, patient advocates, representatives from regulated industry, including companies that sell branded medicines, generic drugs and biosimilars, healthcare organizations, payers and insurers, academic institutions, public interest groups, and the general public.
The background of the notice of the PLS/RFC describes the response to the EO and details certain communications between the USPTO and the FDA in furtherance of its objectives. More specifically, in a letter from the USPTO to the FDA, initiatives for collaboration were outlined including exploring joint USPTO-FDA public engagements, providing examiners with training on publicly available FDA resources, exploring consistency in representations made to the USPTO and the FDA, revisiting patent term extension (PTE) practice, exploring the policies surrounding the use of “skinny labels,” and being open to discussing “patent thickets,” “evergreening,” and “product hopping.”
Further, in the current notice, the USPTO states in a footnote that this collaborative PLS/RFC is in parallel with the USPTO’s initial RFC. The initial RFC included new USPTO initiatives to advance the EO; such initiatives include seeking input on enhancing processes for information disclosure statements and the identification of key prior art, considering applying greater scrutiny to continuation patent applications and use of declaratory evidence during patent prosecution, revisiting terminal disclaimer practice and procedures for third party input during prosecution, and conducting a comparative analysis of the prosecution and grant of “pharmaceutical and biological patents” in the United States versus other countries.
Although the USPTO notice on disclosure requirements and the initial RFC include all technologies, it is clear that the focus of the USPTO/FDA’s inquiries are related to the pharmaceutical and biologics industries.
More specifically, with respect to the PLS/RFC, its inquiries include considering what FDA resources may be available to USPTO examiners to assess patentability, e.g., determining whether inconsistent statements were made to the USPTO and the FDA, using AIA proceedings to address the patentability of claims in pharmaceutical and biotechnological patents, revisiting PTE practices, understanding “skinny label” practice, and generally promoting greater availability of generic products. The PLS/RFC also seeks input on the questions posed in the USPTO letter to the FDA mentioned above.
The in-person PLS at the USPTO is scheduled for January 19, 2023, from 10 am to 5 pm (ET), for which preregistration is needed to speak. Written comments to the PLS/RFC will be accepted until February 6, 2023, with the comments to the initial RFC of the USPTO extended until February 1, 2023.
Stakeholders are encouraged to participate and we will monitor how the USPTO and the FDA respond to these hotly debated topics that impact almost every American.
[1] See 87 FR 45764 (July 29, 2022) and 87 FR 60130 (October 4, 2022), respectively. See also USPTO Publishes Notice Calling Out Pharmaceutical Industry, Goodwin Life Sciences Perspective blog, July 29, 2022; and USPTO Doubles Down Calling Out Pharmaceutical Industry, Goodwin Life Sciences Perspective blog, October 19, 2022, respectively.
 The 340B Drug Pricing Program is a government program, administered by the Health Resources and Services Administration (HRSA), that allows qualifying hospitals and clinics that treat low-income and uninsured patients to buy certain prescription drugs at a steep discount from drug manufacturers. Drug manufacturers participate in the 340B Program as a condition of obtaining Medicaid coverage of their drugs. For the many drug manufacturers who want their products to reach the broadest patient population, participation in the 340B Program is essentially mandatory.
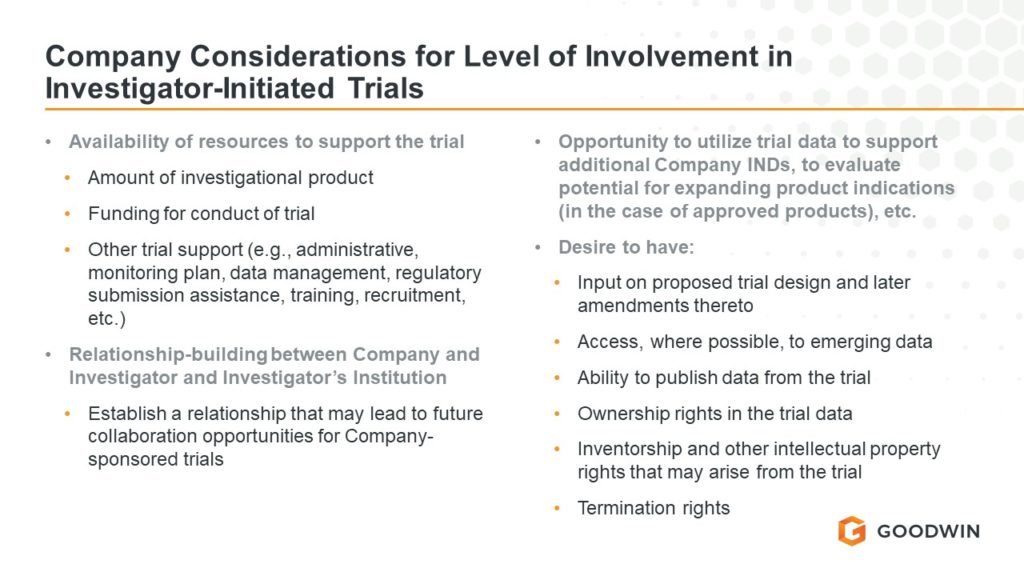
The 340B Drug Pricing Program is a government program, administered by the Health Resources and Services Administration (HRSA), that allows qualifying hospitals and clinics that treat low-income and uninsured patients to buy certain prescription drugs at a steep discount from drug manufacturers. Drug manufacturers participate in the 340B Program as a condition of obtaining Medicaid coverage of their drugs. For the many drug manufacturers who want their products to reach the broadest patient population, participation in the 340B Program is essentially mandatory. For sponsors utilizing a data monitoring committee in their trial designs to monitor for emerging safety signals, lack of effect, and/or futility of treatment, understanding data monitoring committee conflict of interest limitations is important to ensuring an objective view of the data from a trial. Where we see these conflict of interest considerations put to the test most often is in rare disease trials where the available pool of informed experts can be just as small as the patient populations under study. As explained in FDA’s final
For sponsors utilizing a data monitoring committee in their trial designs to monitor for emerging safety signals, lack of effect, and/or futility of treatment, understanding data monitoring committee conflict of interest limitations is important to ensuring an objective view of the data from a trial. Where we see these conflict of interest considerations put to the test most often is in rare disease trials where the available pool of informed experts can be just as small as the patient populations under study. As explained in FDA’s final  … a major change to the Regulation is needed to prevent shortages of life-saving medical devices…
… a major change to the Regulation is needed to prevent shortages of life-saving medical devices…
 The U.S. Patent and Trademark Office (“USPTO”) published a Notice in the Federal Register announcing a new pilot program entitled, “Cancer Moonshot Expedited Examination Pilot Program” (the “Cancer Moonshot Program”) (87 Fed. Reg. 75608 (December 9, 2022)) (the “Notice”) to attempt to further accelerate innovation in the health and medical fields. Beginning on February 1, 2023, this new program will replace the Cancer Immunotherapy Pilot Program and expedite examination for a broader scope of technologies to prevent cancer and advance smoking cessation. The Cancer Moonshot Program is to support President Biden’s recently renewed Cancer Moonshot initiative, which set a new goal of reducing cancer death rate by at least 50% over the next 25 years.
The U.S. Patent and Trademark Office (“USPTO”) published a Notice in the Federal Register announcing a new pilot program entitled, “Cancer Moonshot Expedited Examination Pilot Program” (the “Cancer Moonshot Program”) (87 Fed. Reg. 75608 (December 9, 2022)) (the “Notice”) to attempt to further accelerate innovation in the health and medical fields. Beginning on February 1, 2023, this new program will replace the Cancer Immunotherapy Pilot Program and expedite examination for a broader scope of technologies to prevent cancer and advance smoking cessation. The Cancer Moonshot Program is to support President Biden’s recently renewed Cancer Moonshot initiative, which set a new goal of reducing cancer death rate by at least 50% over the next 25 years. When it comes to discussing medical devices regulated by the U.S. Food and Drug Administration (FDA), words such as “approved” and “cleared” cannot be used interchangeably as these terms carry a particular meaning. Similarly, creating an impression of approval of a device establishment or its devices because the establishment is registered with FDA also is prohibited. Long-standing regulatory provisions,
When it comes to discussing medical devices regulated by the U.S. Food and Drug Administration (FDA), words such as “approved” and “cleared” cannot be used interchangeably as these terms carry a particular meaning. Similarly, creating an impression of approval of a device establishment or its devices because the establishment is registered with FDA also is prohibited. Long-standing regulatory provisions,  The off-label use of ketamine to treat anxiety, depression, and other behavioral health disorders —coupled with the COVID-19 telehealth era—has spurred the opening of virtual ketamine clinics nationwide. Some clinics offer a full suite of health care services, including telehealth visits, prescribing, pharmacy dispensing, and counseling services, while others are focused on more niche areas like group coaching sessions. In the wake of public reports detailing investigations into a number of digital health companies prescribing controlled substances, it is more important than ever to ensure your business model complies with the various regimes regulating the use of ketamine to treat behavioral health issues.
The off-label use of ketamine to treat anxiety, depression, and other behavioral health disorders —coupled with the COVID-19 telehealth era—has spurred the opening of virtual ketamine clinics nationwide. Some clinics offer a full suite of health care services, including telehealth visits, prescribing, pharmacy dispensing, and counseling services, while others are focused on more niche areas like group coaching sessions. In the wake of public reports detailing investigations into a number of digital health companies prescribing controlled substances, it is more important than ever to ensure your business model complies with the various regimes regulating the use of ketamine to treat behavioral health issues. The U.S. Food and Drug Administration’s (“FDA” or “the Agency”) Center for Devices and Radiological Health (“CDRH”) recently announced the launch of its Total Product Life Cycle Advisory Program (“TAP”) Pilot. The first phase of this voluntary initiative, called TAP Pilot Soft Launch, will be conducted during fiscal year (“FY”) 2023 with enrollment beginning on January 1, 2023.
The U.S. Food and Drug Administration’s (“FDA” or “the Agency”) Center for Devices and Radiological Health (“CDRH”) recently announced the launch of its Total Product Life Cycle Advisory Program (“TAP”) Pilot. The first phase of this voluntary initiative, called TAP Pilot Soft Launch, will be conducted during fiscal year (“FY”) 2023 with enrollment beginning on January 1, 2023.