Common GCP Bioresearch Monitoring Violations
 The U.S. Food and Drug Administration’s (FDA’s) Office of Bioresearch Monitoring Operations (OBIMO) oversees domestic and foreign agency field inspections for clinical and non-clinical research. In particular, OBIMO manages the Bioresearch Monitoring (BIMO) Program which conducts onsite field inspections and data monitoring to ensure institution and industry compliance with FDA’s regulations relating to Good Clinical Practices (GCPs). These inspections can occur as a result of a marketing application submission, for general surveillance during an ongoing clinical trial, or as a result of a “for cause” reason. After an inspection, FDA investigators may issue a Form 483 to communicate any onsite findings of noncompliance with FDA’s regulations. BIMO also has authority to issue Warning Letters when the noncompliance FDA identifies is serious.
The U.S. Food and Drug Administration’s (FDA’s) Office of Bioresearch Monitoring Operations (OBIMO) oversees domestic and foreign agency field inspections for clinical and non-clinical research. In particular, OBIMO manages the Bioresearch Monitoring (BIMO) Program which conducts onsite field inspections and data monitoring to ensure institution and industry compliance with FDA’s regulations relating to Good Clinical Practices (GCPs). These inspections can occur as a result of a marketing application submission, for general surveillance during an ongoing clinical trial, or as a result of a “for cause” reason. After an inspection, FDA investigators may issue a Form 483 to communicate any onsite findings of noncompliance with FDA’s regulations. BIMO also has authority to issue Warning Letters when the noncompliance FDA identifies is serious.
In the past 5 years, following are the three most common violations found in OBIMO Warning Letters:
- Failure to ensure that the clinical trial was conducted according to the investigational plan. For example, in one Warning Letter, the FDA noted that a clinical investigator failed to adhere to the investigational plan because subjects took less than the required dosing of the study drug, and some subjects may have taken placebo rather than the required study drug, calling into question the validity of the study data.
- Failure to maintain adequate and accurate study records, including the case histories of individual subjects, the disposition of the drug, or signed informed consent forms. For example, in one Warning Letter, the FDA found that a clinical investigator failed to complete diagnosis summary score sheets for multiple subjects, and the same clinical investigator also failed to accurately report the amount of drug dispensed versus the amount of drug taken by the subject.
- Failure to ensure that proper informed consent was obtained. In several Warning Letters, the FDA determined that the investigators had failed to obtain proper informed consent from participants, including instances where exculpatory language was used waiving the participants’ legal rights, other necessary elements of informed consent were missing, and the form was not specific to the study or approved by the institutional review board.
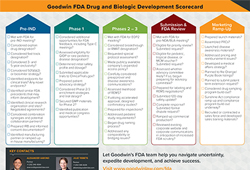
Sponsors and sites should review FDA’s BIMO Compliance Program Guidance Manuals to better understand their responsibilities during clinical trials to ensure GCP compliance and to ensure readiness for future FDA BIMO inspections, should they occur. Anyone who has run a clinical trial will tell you that no trial is perfectly executed; deviations can and will occur, so preparedness is necessary. An effective monitoring program is critical to sponsors ultimately ensuring the integrity of their clinical trial records and data set. The Goodwin FDA Regulatory team works closely with sponsors on managing GCP issues when they arise during clinical trials.
Connect with our Goodwin FDA team to learn more.
*Madeline Fuller, a 2021 summer associate in Goodwin’s Washington, D.C. office, contributed to this post.
 On January 19, 2021, the FDA issued
On January 19, 2021, the FDA issued  As follow-up to our October
As follow-up to our October  In this post, we discuss FDA’s conduct of inspections of manufacturing facilities for new drugs and biologics during the COVID-19 pandemic. These inspections, known as pre-approval and pre-licensure inspections (PAIs/PLIs, respectively), are performed to give FDA assurance that a manufacturing site named in a new drug or biologics license application is capable of manufacturing the product according to current good manufacturing practices (cGMPs) and producing the product at commercial scale.
In this post, we discuss FDA’s conduct of inspections of manufacturing facilities for new drugs and biologics during the COVID-19 pandemic. These inspections, known as pre-approval and pre-licensure inspections (PAIs/PLIs, respectively), are performed to give FDA assurance that a manufacturing site named in a new drug or biologics license application is capable of manufacturing the product according to current good manufacturing practices (cGMPs) and producing the product at commercial scale.